How has malaria resistance spread in South-East Asia?
So far, the resistance of malaria parasites to artemisinin—the main component of the best available antimalarial ttreatments—has been detected in six countries in the Greater Mekong region: Myanmar, Cambodia, China, Laos, Thailand, and Vietnam. If nothing is done to contain resistance, it risks spreading westwards, into India, even as far as Africa, which would have catastrophic consequences. Early efforts to contain the issue within the borders were not entirely successful, as people continued to travel from country to country, and they carried resistant strains with them. So, we changed our approach. We are now aiming for the total eradication of the resistant strain throughout the region.
How can regional initiatives like RAI respond to this issue?
Resistance issues like those affecting the Greater Mekong region require a coordinated regional response.
Resistance issues like those affecting the Greater Mekong region require a coordinated regional response. All of these countries are facing similar challenges—migration, ethnic minority problems, hard-to-reach areas—and can benefit from similar solutions. RAI coordinates the surveillance of malaria cases, including those crossing borders, and ensures that all countries follow recommendations. All this is possible thanks to a strong network of partners, including the WHO regional office in Phnom Penh, brought together under the supervision of RAI, and a coordination platform of civil society organizations in the region.
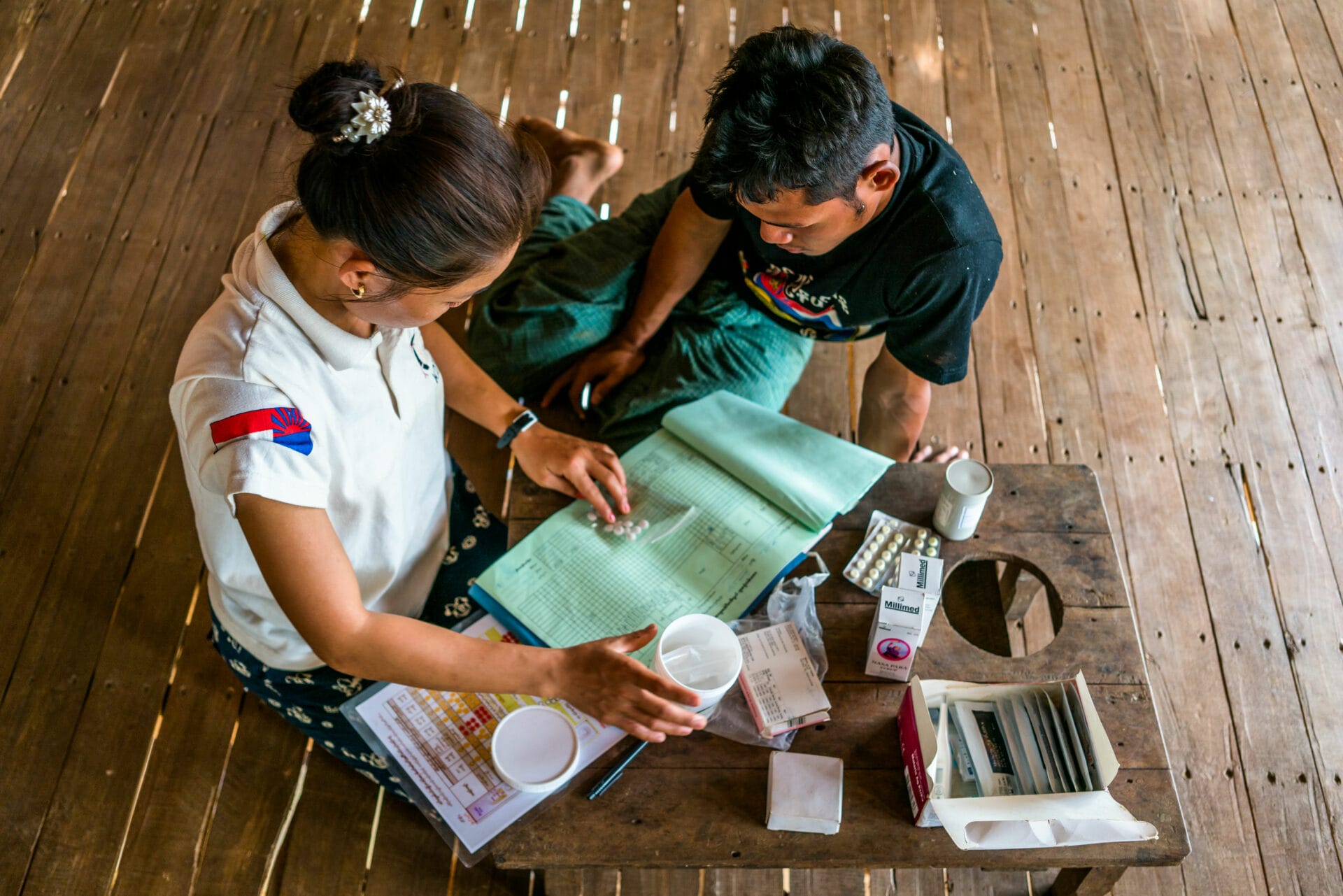
The work of these organizations is invaluable to us, especially in areas controlled by ethnic minorities and hard-to-reach areas. We also support a network of around 40,000 volunteers at the village level, who screen and treat their communities. Detected malaria cases are then reported on a smartphone application that feeds into the national database in real time. This complex management of malaria information has proven to be crucial for the surveillance of cases in the region and to facilitate a rapid response in the event of an epidemic.
What have been the positive results of this approach?
It now appears possible to eradicate Plasmodium falciparum in the six countries by 2023.
For years, the eradication of Plasmodium falciparum, the strain of the disease susceptible to developing resistance, was unimaginable. And yet, this is exactly what is happening. We have seen malaria cases drop dramatically in every country where RAI is active. It now appears possible to eradicate Plasmodium falciparum in the six countries by 2023.Until recently, we were aiming for 2025 or even 2030. Never in the history of the disease has it been possible to eradicate malaria from an entire region so quickly. It is a historic achievement.
To what extent has L’Initiative’s technical assistance contributed to this success?
Since RAI was established, L’ Initiative has been a crucial partner. It has systematically made the necessary resources available to recruit high-level consultants to support its funding requests. Since 2013, we have launched three fundraising campaigns, and L’Initiative has responded every time. L’Initiative was particularly generous in the last campaign, funding a large number of consultants who are now helping us at national and regional levels.
Can this model of cooperation and coordination be applied to other health challenges or other regions of the world?
We want to share our good practices with regions in the same situation, such as Southern Africa.
Absolutely. We want to share our good practices with regions in the same situation, such as Southern Africa. In Southern Africa, eight countries face similar problems of migration, accessibility, and ethnic tensions without necessarily having the same socio-economic context. To cooperate effectively in the response to malaria, countries in this region could benefit from a regional data management system, the deployment of volunteers, and the creation of a high-level coordinating institution to oversee progress.